Course
Understanding the Types of Anemia
Course Highlights
- In this course we will learn about the various types of anemia and their specific lab values.
- You’ll also learn the basics of red blood cell production.
- You’ll leave this course with a broader understanding of interpretting key lab values that indicate anemia.
About
Contact Hours Awarded: 1.5

Course By:
Ashley Kellish
DNP, RN, CCNS
Begin Now
Read Course | Complete Survey | Claim Credit
➀ Read and Learn
The following course content
Anemia remains a common and complex diagnosis in the healthcare setting. From relative anemias subsequent to fluid overload or dehydration, to true anemia secondary to illness or related to a genetic disorder, a nurse is never far from an anemia diagnosis. That said, we can enhance our ability to describe and determine the various types of anemia based on digging deeper into the lab values that exist with anemia.
Introduction
Anemia, by definition, is a decrease in circulating red blood cells (RBCs) and a decrease in Hb concentrations in the blood (2). The human body makes 2 million RBCs per second. The RBC is constantly regulated by blood concentration passing through the kidneys (2). When the hemoglobin is low, the kidneys secrete erythropoietin which sends a message to the bone marrow to produce more RBCs. Because our body needs certain nutritional requirements to make RBCs appropriately, like iron required for the synthesis of Hemoglobin, B12, folate, B6, riboflavin, pantothenic acid, niacin, ascorbic acid, and vitamin E, deficiencies in these elements can cause anemias (2).
In particular, folate and B12 are absorbed from food in our ileus in the gut. Folate and B12 deficiencies lead to impaired DNA synthesis in erythroid cells in the bone marrow during production. Erythroid cells are the beginning cells of RBCs (1, 2). Cells that are lacking folate and B12 are shown to be too small on the microscope because they never fully form. Additionally, B12 requires intrinsic factor (IF) found in gastric juice secreted by parietal cells. Therefore, a decrease in B12 can lead to anemias when IF is not available in the gut (1, 2). Although this may seem complicated, the key point is to recognize that anemia is not simply related to a low number of RBCs, but there are many facets that can lead to anemia in our bodies and based on overall health.
RBC Production
RBCs are produced in the bone marrow (2). Pluripotent stem cells differentiate into either myeloid or lymphoid stem cells. Lymphoid stem cells differentiate further into lymphocytes, while myeloid cells differentiate into erythrocytes, thrombocytes, granulocytes, and macrophages. Erythrocytes are what eventually become RBCs. The most interesting part is that when an erythrocyte differentiates into a reticulocyte or immature RBC, this is what is initially released into the bloodstream (2). At this point, it has no nucleus-very different than most cells!
Reticulocytes, or immature RBCs, still have another 24-48 hours of development to undergo before they are a mature and functioning RBC. During this time, they lose their mitochondria and ribosomes as well. They make up 1% of the total RBCs (2).
With these typical cell organelles missing, the RBC makes and uses energy, or ATP, in a very different way than the typical cell. RBCs have a lifespan of 120 days and undergo a very formal destruction process that allows our body to recycle certain parts of the RBC for later use (2, 4).
As an RBC ages, enzyme activities decrease, membrane lipids decrease, allowing for instability due to the rise of destructive elements like HBA and methylhemoglobin.
Changes in cell size occur, and then the cell becomes increasingly fragile and removed by the mononuclear phagocytic system. 80-90% of this process occurs in the liver and spleen, where the globulin and iron stores can be recycled while the heme is reduced to bilirubin (2, 4, & 5). The bilirubin is broken down into urobilinogen and excreted in our feces (giving it a brown color!). The increased red cell destruction can show an increase in serum levels of unconjugated bilirubin and increased excretion of urobilinogen which can be indicative of an RBC destruction issue and therefore anemia (4).
Symptoms of Types of Anemia
Anemias can have many symptoms, but there are some common ones to look out for (3). In addition to these, anemias symptoms can be masked by chronic illnesses so keep that in mind during patient assessments. The common symptoms include fatigue, pallor, weakness, yellowish or jaundiced skin, irregular heartbeats, shortness of breath, dizziness, chest pain, cold hands and feet, headaches, and paresthesias (2). The numbness and tingling are often associated with other neurological changes, indicating a B12 deficiency (1). It is important to take a good history and determine the length of time the patient has had these symptoms, and monitor lab values to help in diagnosis. The best part is that the various types of anemia can be treated most of the time with simple measures and follow-up to ensure the anemia is resolved.
Key Lab Values for Types of Anemia
Most of the time, when we measure a “retic” count, we are ensuring there is normal bone marrow function. A high retic count would be evidence of too many immature RBCs in our bloodstream, and the opposite is true with the reverse (2). These lab values can be indicative of anemia.
Check out the chart below (2) for some key lab values and their normal values when looking at types of anemia. Note the highlighted MCV and MCHC which show the size and color of RBCs. These lab values are vitally important when reviewing a patient’s Complete Blood Count (CBC) and looking for what type of anemia it may be.
| Indices | Description | Normal Range |
| RBC: Red blood cell count | Total # of RBCs in blood |
|
| Hemaglobin (Hgb) | Concentration of Hgb in blood |
|
| Hematocrit (Hct) | Volume of packed RBC |
|
| Mean RBC Volume (MCV) | Average size of RBC |
|
| Mean Cell Hemoglobin Concentration (MCHC) | Concentration of Hgb in the average RBC |
|

Self Quiz
Ask yourself...
What did the last patient you cared for have along with anemia?
Have you ever been anemic yourself and been told you should take vitamins/supplements?
Types of Anemia Based on Lab Values
Use the following flow charts to learn the names and types of the more common anemias in response to the lab values a patient presents with. Learning how the lab values can dictate the anemia presented is a useful tool when you are caring for patients.
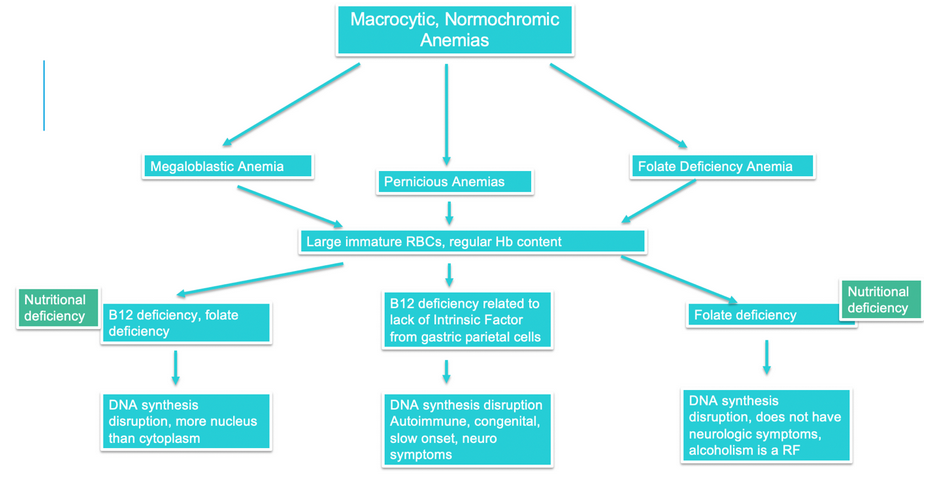
A macrocytic, normochromic anemia, by definition, is one in which the RBCs are too large but have a normal amount of hemoglobin. This would be evidenced by a high MCV and normal MCHC.
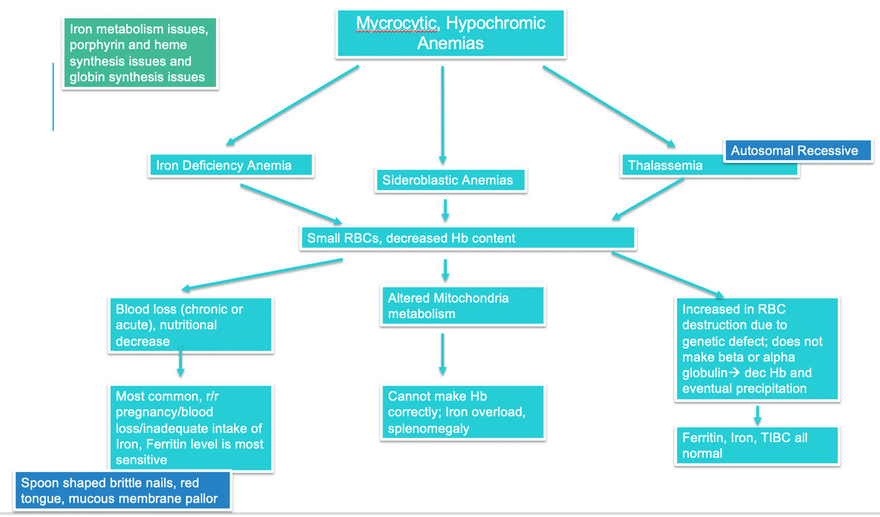
In contrast, a microcytic, hypochromic anemia would be evidenced by a low MCV and low MCHC. Check out the charts for what types of anemia are characterized by these lab values (2).
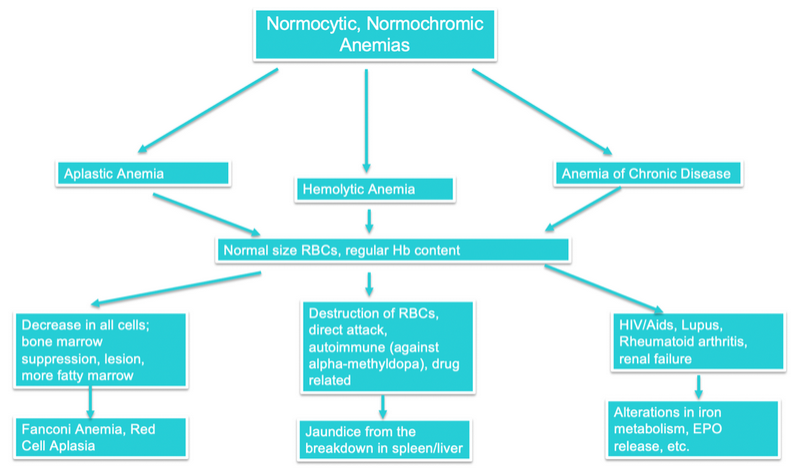
However, it is important to note that there are anemias that represent a failed destruction process, and too many RBCs are destroyed, leaving the body anemic. These are called hemolytic anemias or aplastic anemia (2, 4). In both, RBCs are destroyed at rates too high for the body to recover.
In aplastic anemia, all cells made by the myeloid stem cell in the bone marrow are rapidly destroyed, and this is how you can identify this anemia over others.
Self Quiz
Ask yourself...
- Using the charts above, determine what type of anemia someone has if they present with a high MCV, a normal MCHC, and low B12 and low folate due to a lack of intrinsic factor.
- Using the charts above, determine what type of anemia someone has with a normal MCV, normal MCHC but jaundiced and fatigued.
Case Study #1
A 42-year-old female presents to the emergency department with fatigue, pallor, cracked lips, a swollen tongue, and paresthesias. On discussion, you learn that she had gastric bypass surgery about two months ago. She was sent home with limited ability to get to follow-up appointments due to a lack of a car and support system. You know gastric bypass surgery can interrupt normal gastric function, and you are reminded of the parietal cells’ secretion of intrinsic factor necessary for B12 absorption. This is starting to sound like anemia related to deficiencies, but you need to confirm via labs. Her lab values are as follows:
- Hgb: 9
- MCV: 130
- MCHC: 34
Out of the various types of anemia, which do you believe she is suffering from?
Provide the type and summarize the morphology and pathophysiology.
Case Study #2
A 68-year-old gentleman presents to the emergency room with a blunted affect mirroring depression, sleep deprivation, memory loss, personality changes, and irritability. You find out during your assessment that he has a history of intermittent heavy alcohol use. You know heavy alcohol consumption can cause a decrease in normal vitamins and minerals, and you ask him about his nutritional status. It is not good. His lab values are as follows:
- Hgb: 9
- MCV: 130
- MCHC: 34
What type of anemia is he suffering from?
Provide the type and summarize the morphology and pathophysiology.
Conclusion
Anemia is a common cause for hospitalization and a common post-hospital complication. As nurses, looking beyond the hemoglobin and hematocrit values can help us work with our teams to assess and care for patients with anemia. Patients can be treated appropriately when diagnosed properly and swiftly, either in clinic or emergency department settings. The next time you care for a patient with anemia, look at their labs with a deeper understanding of what is happening at the production and/or destruction level.
References + Disclaimer
- Anemia, Pernicious. (2005). Rare disease database. Retrieved from: https://rarediseases.org/rare-diseases/anemia-pernicious/.
- Banasik, J & Copstead, L. (2019). Pathophysiology, 6th edition. Elsevier Inc..
- Brugnara, C. (2003). Iron deficiency and erythropoiesis: new diagnostic approaches. Clinical Chemistry, 49(10). 1573-1578.
- Mass General Hospital (2016). How the body disposes of red blood cells, recycles iron. Retrieved from: https://www.sciencedaily.com/releases/2016/07/160718132646.htm
- Wallace, D. (2016). The regulation of iron absorption and homeostasis. Clinical Biochemi Rev., 37(2). 51-62.
Disclaimer:
Use of Course Content. The courses provided by NCC are based on industry knowledge and input from professional nurses, experts, practitioners, and other individuals and institutions. The information presented in this course is intended solely for the use of healthcare professionals taking this course, for credit, from NCC. The information is designed to assist healthcare professionals, including nurses, in addressing issues associated with healthcare. The information provided in this course is general in nature and is not designed to address any specific situation. This publication in no way absolves facilities of their responsibility for the appropriate orientation of healthcare professionals. Hospitals or other organizations using this publication as a part of their own orientation processes should review the contents of this publication to ensure accuracy and compliance before using this publication. Knowledge, procedures or insight gained from the Student in the course of taking classes provided by NCC may be used at the Student’s discretion during their course of work or otherwise in a professional capacity. The Student understands and agrees that NCC shall not be held liable for any acts, errors, advice or omissions provided by the Student based on knowledge or advice acquired by NCC. The Student is solely responsible for his/her own actions, even if information and/or education was acquired from a NCC course pertaining to that action or actions. By clicking “complete” you are agreeing to these terms of use.
➁ Complete Survey
Give us your thoughts and feedback
➂ Click Complete
To receive your certificate