Course
The Basics of Wound Healing
Course Highlights
- In this course we will learn about the various types of wounds, and why it is important for nurses to be prepared on how to effectively treat them.
- You’ll also learn the basics of wound healing phases, assessments, and management.
- You’ll leave this course with a broader understanding of how to properly care for wounds and evaluate their healing status.
About
Contact Hours Awarded: 3
Course By:
Melody Heffline
MSN, APRN, ACNS-BC, ACNP-BC, ACHPN
Begin Now
Read Course | Complete Survey | Claim Credit
➀ Read and Learn
The following course content
In the world of nursing, wounds have become a common area of need for understanding. Wounds can be fairly simple to care for or very complex in nature. This presentation will provide information on types of wounds encountered in nursing practice; wound healing and how this occurs; what can impair the healing process and how to improve wound healing by addressing these factors; and steps in the management of the various types of wounds, including choosing the right dressing. A case study will be used to aid in understanding wounds and their management.
Introduction
Wounds! Just the word can strike terror into some of our hearts. However, once you get to know them, you can relax and use what you know to give them the best care possible. So come along with me, and let’s break down the basics of wound healing together! Hopefully, you will learn to love them as I have, because nurse colleagues, they are here to stay and become more common every day. On top of this, they are very costly to the healthcare system. Wounds can cross over many areas of nursing, so no matter where you practice, chances are, you will encounter a wound and need to know how to care for it. Let’s journey into the types of wounds we may see, what hinders them from healing, how to attack those hindrances, and how to manage wounds to get them to the finish line!
Case Study
Let’s meet our patient, Ms. E, that we will look at throughout this lesson.
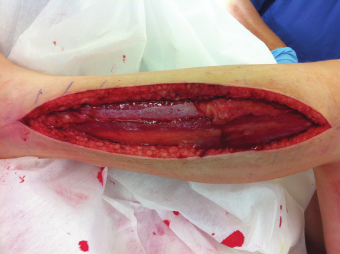
She is a 56 year-old female with peripheral arterial disease who developed an arterial thrombus in her right lower extremity. Unfortunately, though she responded to thrombolytic therapy and flow was restored to her leg, it did not happen before she developed compartment syndrome in her leg requiring fasciotomy. Her medial incision was able to be closed in a delayed fashion about 48 hours after the surgery. However, she still had a significant amount of edema in the leg, and the lateral incision had to be left open to granulate by secondary intention. Her past medical history includes COPD, diabetes mellitus with hyperglycemia, tobacco dependence, smoking two packs per day at the time of her event, morbid obesity with BMI 50.7, CAD with previous MI, and coronary stent placement. Blood sugars at the time of the event were running in the 200-300 range with an A1C of 10.3. She has frequent exacerbations of her COPD, requiring steroids and antibiotics. She has significant edema in the lower extremities due to a lack of elevation. She is allergic to ciprofloxacin, cephalexin, levofloxacin, and latex. She was started on warfarin following thrombolysis of the thrombus, but due to significant issues with attempting to stabilize her INR, she was switched to apixaban twice daily and clopidogrel daily. To say the least, getting this very large fasciotomy wound to heal will be challenging.
Wound Type
In order to develop a thorough understanding of wound healing, let’s start with a simple definition of a wound. A wound happens when the skin is traumatically disrupted. This can occur in a controlled fashion such as with surgery or in a more traumatic fashion such as bites from pets or other animals, gunshots, or lacerations, creating a jagged-edged wound.
Surgical Wounds
Surgical wounds may be further classified into wounds that are:
- Clean (uninfected)
- Clean-contaminated (in the respiratory, GI, GU tract)
- Contaminated (the result of trauma or loss of sterile technique)
- Dirty (infected)
When a wound is clean or clean-contaminated, it can be closed at the end of a surgical procedure. If a wound is contaminated or dirty, it is usually left open at the end of the surgery because its bacterial burden is too high. To close this wound is generally futile because it would lead to infection. This wound can be better managed if left open. Wounds closed surgically are defined as primary closure. Wounds are left open to heal by secondary intention, allowing granulation tissue to form and eventually allowing the wound to close. Some wounds can be left open to allow for treatment of infection and then closed in a delayed fashion (1, 2). This is the case with Ms. E’s wound.
It is common to take care of the patient with primary closure. Have you seen the wound that is allowed to heal by granulation?
What types of problems did you encounter with this patient? How long did these wounds take to heal?
Wounds may be larger such as those that happen from auto accidents where we see crush injuries, traumatic amputation, or even burns and thermal injuries. Initially, wounds are classified as acute, and the hope is that they heal quickly. But what about lack of blood flow? When blood flow is disrupted in an area, wounds can happen because tissue breaks down if there is insufficient blood flow to keep the skin alive in a particular area(1).
What may be happening to cause blood flow to be impaired and cause a wound?
What other complications can occur where there is insufficient blood flow?
When lack of blood flow is an issue, usually we are talking about poor arterial circulation to an area. Patients may do well for a while as long as skin is intact and there is no trauma, but with impaired arterial flow as with atherosclerosis, the tissue will not survive indefinitely. It may break down on its own. Blood vessels can become compressed such as with a hematoma, where a large collection of blood forms under the skin from blunt force trauma or surgical bleeding issues. The hematoma enlarges and compresses arteries under the skin leading to decreased blood flow. In Ms. E’s case, severe edema due to muscle ischemia led to severe edema. The skin then may start to die, leading to breakdown and wound development, or may require a fasciotomy to relieve pressure and save the muscle from certain death.
Arterial Ulcers
Arterial ulcers can develop and be very challenging to heal. Arterial ulcers have a characteristic of a “punched out” appearance and are pale in the base, indicating the lack of blood flow; additionally, they tend to be dry in the base with little moisture. Usually, they are very painful for the patient, partially due to the location over a bony area and the lack of blood flow. Arterial ulcers can also present as wet or dry gangrene (1). Though Ms. E’s wound is not now classified as an arterial wound, it started as a result of a lack of blood flow in her extremity. Only the restoration of blood flow saved her from an amputation.

Have you ever fallen asleep on your arm or leg and felt the pain of the lack of circulation when you woke up?
Consider the pain in an extremity where blood flow cannot be restored simply by moving the extremity and readjusting its position.
Venous Ulcers
Another type of ulcer that can develop is a venous ulcer. Venous ulcers develop as a result of longstanding venous insufficiency; this happens when valves fail or become incompetent in the lower extremity. Venous ulcers have a ruddy appearance and very irregular edges. They produce a lot of drainage or exudate. These ulcers can range from extremely painful to having little sensation if they have been present for a long period (1, 2).
Neuropathic Ulcers
Although neuropathic ulcers are typically found in diabetic patients, not everyone who develops neuropathy is diabetic. However, their cause is the same – lack of sensation in the area – usually the foot. They can occur anywhere on the foot but are more common over bony areas and most often happen because of friction and repeated trauma in the area; there are usually calluses in these areas, as a callus is a response to repeated trauma. The body is trying to protect the underlying tissue by becoming hard and thick. When the body does not feel this happening, it leads to additional trauma and tissue breakdown. Think of putting a rock in the shoe and walking on it all day long. You would know that damage was occurring. These patients are experiencing this, but they don’t feel it because they have lost the protection of having sensation in the foot. These ulcers are usually round and can be shallow or deep, depending on the trauma to underlying tissue. Often, the depth is unknown until the surface of the wound is removed to reveal the extent of the wound. The perimeter of these wounds may be made up of hard callus. The base of this wound may be pale if the arterial disease is present, or it can be a more beefy red tone (1).

Pressure Ulcers
Pressure ulcers occur as a result of pressure to an area of skin, resulting in injury to deeper structures; immobility is a common cause. They are usually present over bony prominences that have been against a bed, or perhaps a wheelchair. This reduces circulation to the area and may cause tissue death if the pressure is not relieved. Friction can also contribute to pressure ulcers, such as when sliding up in bed or using a heel to push up in bed. Pressure ulcers may result in deep tissue death and are classified in stages from one to four.
- Stage 1 is characterized by erythema that does not blanch with pressure.
- Stage 2 is indicated by partial skin thickness tissue loss with a shallow opening and a red wound base.
- Stage 3 ulcers show full-thickness tissue loss with exposed subcutaneous tissue.
- Stage 4 ulcers reveal exposed bone, tendon, and muscle tissue (1, 2)
What nursing measures are needed for the patient who spends most of their time immobilized to prevent pressure ulcers?
What medical equipment may help in these endeavors?
What challenges present themselves when a patient no longer has sensation in the feet? How do you address these challenges?
There is no designated timeline for wound healing, and there is no determination of when a wound is to be labeled as chronic or acute; however, generally, wounds that don’t heal within a few weeks tend to be viewed as chronic. Ideally, wounds should decrease in size by 50% in the first four weeks. If this is not the case, it is more than likely that something is causing the delayed wound healing. Wounds should be showing signs of healing with every passing week, and if they aren’t, an investigation into why should be started (1).

Self Quiz
Ask yourself...
Have you cared for a wound that is healing well, and all of a sudden, it is no longer progressing?
What makes a wound heal normally and then stop progressing?
What might be going on with the patient?
Case Study (cont.)
Ms. E’s wound was large, measuring over 26 cm in length and 11 mm in width. She had an exposed tendon in the wound. Due to the size of the wound and the edema that led to large amounts of exudate, she was started on negative pressure wound therapy (NPWT) from the beginning of her treatment. She developed significant skin excoriation initially due to the large amounts of drainage her skin was exposed to. She was not adherent to the plan of care, which required her to keep the leg elevated to help control edema, and edema was a big contributor to lack of healing. The decision was made to begin treatment with a skin substitute to improve the chances of healing the wound. The product chosen for her was Kerecis. We’ll talk about this product later.
Self Quiz
Ask yourself...
Thinking back to her history, what other things may be causing this wound’s lack of progression besides the edema?
Normal Wound Healing Phases
Before we look at what hinders wound healing, let’s look at the normal wound healing process.
Inflammatory Phase
The initial phase of wound healing is known as the initiation or inflammatory phase; usually, it lasts one to five days. Upon injury, the vessels in the skin will constrict to provide for hemostasis and limit bleeding. The clotting cascade is triggered after the platelets begin to aggregate or clump together; this sets up the release of growth factors and plays an important role in wound healing progression. A fibrin matrix will form as the basic structure around which the wound can heal. If the wound involves larger vessels, pressure may be needed to control bleeding. In some cases, other agents may be needed to produce hemostasis and control bleeding (1, 2).
We may tend to think of inflammation as a sign that something is wrong, but this is a part of normal wound healing. This phase does not produce a strong wound and is usually complete in around three days unless the wound becomes infected or something else interferes with the healing process. This phase includes macrophage development, degranulation of mast cells, and histamine release, which causes vasodilation. This is the phase where swelling may be seen and occurs due to the permeability of the vessels from the cellular mediators that are present.
Epithelialization Phase
The next phase of wound healing involves epithelialization. In this phase, basal cell and epithelial cells work to develop a fibrin network of similar cells; this process stops when the dermal layer of cells is rebuilt. In a surgical wound, this process may take as little as 48 hours. This layer forms a protective layer to help keep out bacteria and foreign bodies. This layer is fragile and can be easily broken with trauma to the wound if a wound is not primarily closed where the edges are brought together and closed. Wounds that have to heal by secondary intention take longer, as the migration of the epithelial cells must reach across a larger surface area. In these wounds, a substance known as biofilm can develop. Biofilm is produced by bacteria that bind to the wound base and leads to ongoing inflammation and impair the epithelialization process. Epithelial cells may also become inactive, making them unable to replicate. They cannot proliferate or reproduce rapidly, further impairing the healing process (1,2).
Proliferation Phase
The next phase of wound healing is the stage of fibroplasia or proliferation. This phase can last from two to 20 days. In this phase, fibroblasts will proliferate, ground substance accumulates, and collagen will be produced. Fibroblasts are usually in the wound in the first 24 hours. They work by attaching to the clot’s fibrin matrix and produce proteins called myofibroblasts. These are usually present in the wound by the fifth day. The ground substance is made up of glycoproteins, mucopolysaccharides, electrolytes, and water. The process of apoptosis (programmed cell death) leads to the loss of the myofibroblasts as the wound forms a scar. Collagen formation is also done by fibroblasts and continues for up to six weeks following a surgical wound. This stimulates angiogenesis, or the formation of new blood vessels. The combination of collagen production and angiogenesis leads to granulation tissue formation. When there is abnormal fibrosis, extensive scarring can happen and leads to a keloid; this may be visible in the wound during the healing process as hypergranulation tissue (1, 2).
Remodeling Phase
The final phase of wound healing is that of a mature wound and is sometimes called the remodeling phase. This phase of healing can extend from 21 days to months or years. The final strength of the wound will be related to the collagen present in the wound. Collagen will need to cross-link and remodel for the wound to mature. In a surgical wound, about 80 percent of the original tissue strength is present in 6 weeks. The wound, however, will continue to heal for up to 180 days. This skin may get stronger but will never regain its full, previous strength. Factors that influence the final strength include the severity of the initial wound and any delay in wound healing that occurs. Some wounds will be remodeling for years following surgery or trauma (1).
Self Quiz
Ask yourself...
What wounds have you taken care of that have progressed normally?
Can you recall the wound passing through the stages we have just discussed?
Did those wounds heal primarily or secondarily?
Impaired Wound Healing
Many factors can contribute to poor wound healing. Knowing the risk factors for impaired wound healing and how to address them will help speed up the healing process and shorten the time a patient has to contend with an open wound. Let’s look at some of the factors that may occur and how each one may be treated to reduce the time it takes for a wound to heal.
What critical issue must be resolved for a wound to have a chance to heal?
Blood Flow
A wound cannot heal without proper blood flow. Think about all those chemical mediators that are a part of normal wound healing that we have just discussed. They arrive in the tissues via circulation carried in the blood along with oxygen. Oxygen-deprived tissue will not heal, and the lack of blood flow also affects the removal of metabolic waste products. No matter where a wound is located, it will not heal if there is insufficient blood flow.
This may require intervention to restore blood flow, such as a bypass, endarterectomy, angioplasty, or stenting for wounds located on an extremity; this may be necessary in the arterial wound or in the diabetic/neuropathic ulcer. Atherosclerosis is common in diabetic patients. Patients who complain of pain, tiredness, cramping, or a “giving way” sensation when walking may be experiencing claudication, which occurs when the demand for blood in the extremity muscle cannot be met due to impaired blood flow in the extremity.
When wounds are already present, there is an even greater need for blood flow. Rest pain occurs when there is insufficient blood flow at rest in the extremity. This patient’s wound can progress to ischemia quickly and will need urgent restoration of blood flow to heal a wound. Patient education involves teaching the patient to protect the limb from injury and reporting any signs of worsening circulation, including increased pain, color changes in the extremity, wearing proper footwear, and never going barefoot. They will also need help in modifying the risk factors associated with the development of arterial disease (2, 3).
Infection
An infection will impair wound healing at several steps along the way. If bacteria are in the wound, the inflammatory phase of wound healing is impaired, preventing epithelization from occurring; cells may die, increasing inflammation in the wound. Necrotic tissue will develop and will hinder new tissue from forming. The formation of necrotic tissue can also lead to further bacteria in the wound resulting in a cycle of non-healing. Think back to the types of surgical wounds we talked about earlier; the degree of contamination of a surgical wound at the time of incision will play a role in ongoing infection. The presence of cellulitis or skin infection can slow the healing process of the wound. This is a common occurrence with venous ulcers due to edema, which allows bacteria to enter microscopic tears in the skin. Burn patients are at high risk of infection, especially if a large percentage of skin is lost. Thermal injuries may be accompanied by an immunosuppression response as well.
The nurse’s role in educating patients about keeping wounds as clean as possible is critical to preventing contamination in the home. Teach them to keep them covered and avoid contamination by pets when changing bandages. For a wound to be classified as infected, it should have purulent material (cloudy fluid). A positive wound culture in a wound that was closed in a primary fashion and has reopened indicates infection. Infection may be superficial or involve deep infection into an organ or wound space. These wounds will require treatment with antibiotics. Cultures are only obtained in chronic wounds if they have signs of infection, such as heavy purulence or excessive drainage, and other signs of infection such as cellulitis around the wound. Random cultures will be positive for bacteria once the wound becomes chronic as there will be microbes in all wounds, but all wounds are not considered infected. Cultures should always be obtained following debridement to penetrate the biofilm, which will yield more accurate results. Excessive use of antibiotics can lead to resistant bacteria and the development of allergies (2, 3, 4, 5).
Smoking
Smoking has been linked to surgical site infections but may also interfere with wound healing by other mechanisms. Some of these mechanisms are not fully understood. Nicotine has been presumed to be the major contributor to the impairment, but more recently, the compounds in the smoke are believed to play a role. The Department of Health and Human Services states that there are over 7,000 chemicals in tobacco smoke. Some of them include carbon monoxide, arsenic, hydrogen cyanide, formaldehyde, benzene, lead, and mercury. Look up some of these chemicals to find out more about what they do in the human body over time. Multiple factors are to blame for the detrimental effect of smoking, but the vasoactive effects of nicotine, which leads to ischemia by vasoconstriction, will also reduce the inflammatory response.
This alters the destruction of bacteria and collagen metabolism, these effects lead to wound dehiscence as well as incisional hernias. Studies have shown that even stopping smoking four to eight weeks before surgery can improve wound healing and decrease surgical site infections. Of note, smoking can reduce blood flow by up to 40%, with the effects lasting up to 45 minutes. For patients who smoke a pack a day or more, this can certainly add up to a significant reduction in blood flow to vulnerable tissue. Studies using nicotine replacement therapies (NRT) for tobacco cessation have not shown these same effects. It may be useful in wound patients to try using NRT in combination with other methods to help them stop tobacco use. Patient education regarding these effects is critical in gaining the patient’s participation in promoting their own wound healing (2, 3, 5, 6).
Case Study Update
Ms. E presents many challenges, but the significance of her tobacco abuse is a big contributor to her wound’s stalling. With encouragement at every office visit, she eventually has gotten to one pack a day but shows little interest in eliminating tobacco use. This is one of the greatest challenges in wound care because the patient must see the need for the modification of this risk factor. Tobacco cessation not only involves the withdrawal from a powerful chemical in the body but also helping the patient with the habit and the things they do that are associated with lighting up a cigarette. Unless she comes to the place where she wants to stop smoking, this barrier to wound healing may never be resolved.
Aging
The aging process will affect the skin as nerves and blood vessels in the skin decrease with age. The layers of the skin also will thin with age from the dermis through to the basement membrane. There is a loss of collagen, and the ability to produce collagen decreases as well; this can lead to slower healing as well as wound breakdown from infection. Unfortunately, this is a risk factor that cannot be changed. In older patients, it’s vital that education is provided to help change the risks that can be modified (2).
Nutrition
Nutrition plays a vital role in wound healing. Proper nutrition should ideally come from the diet as there is not a great deal of evidence supporting the use of dietary supplements. Supplements that have been used with some success include zinc and vitamin C. Encouraging increased protein intake may also aid in the wound healing process (2, 3).
Immobilization
Prolonged immobilization increases the risk for the development of wounds, especially pressure wounds. In some wounds, immobilization can help with wound healing, such as in the case of boots and casts for foot ulcers. Patients should be instructed on the importance of position changes to prevent pressure areas on the back, sacrum, and heels where pressure ulcer development is common (2, 3).
Self Quiz
Ask yourself...
- What changes are present in the lower extremities besides pain that can give clues that PAD might be present and contributing to poor wound healing?
- Should all wounds with bacteria in them be treated with antibiotics? What options may need to be considered when a patient such as Ms. E has allergies to the antibiotics needed to treat her wound infection?
- What are other methods that may be used to help smokers quit the use of tobacco?
What issues can occur in the aging patient with a poor appetite who is also immobilized?
What might additional education be necessary for these patients?
Impaired Wound Healing (cont.)
Diabetes
Diabetes has long been known to have an adverse effect on wound healing. There are many ways that diabetes impairs wound healing at the cellular level:
- Reduction in growth factors
- Decreased angiogenesis
- Decreased macrophage production
- Decreased collagen synthesis
- Impaired function at the epidermal layer, including number of nerves
- Decreased granulation tissue
- Decreased fibroblast migration and proliferation
- Decreased bone healing
- Lack of balance between extracellular matrix components and remodeling by matrix metalloproteinases (MMPs)
Diabetes contributes to the development of neuropathy and vascular disease from atherosclerosis. Both conditions increase the chances that infection will develop, and wound healing will be delayed. Peripheral arterial disease (PAD) with neuropathy leads to the development of foot ulcers and can lead to limb loss from non-healing. The loss of sensation from neuropathy leads to the loss of pain perception and unawareness of injury.
Many patients with diabetes will develop bony changes of the toes and midfoot, and the arch of the foot collapses. These bony changes combined with the loss of sensation lead to skin breakdown from improper footwear in weight-bearing locations. Loss of autonomic nerves leads to dry skin that is more susceptible to breakdown and tearing as the patient loses sweat and oil gland function. It is imperative that patients are provided education on controlling diabetes and the importance of foot care, including foot examination daily and proper footwear that is replaced annually.
Case Study Update
Due to her diabetes and constant hyperglycemia, Ms. E has had issues with infection that have required treatment. Due to her COPD exacerbations and pneumonia, she has required multiple rounds of steroids which have contributed to her lack of diabetes control. Her A1C is now 12 and her blood sugars are running in the 250-300 range most days. Ms. E often says, “I know I don’t eat like I should.”
Venous Disease
Venous insufficiency contributes to the development of venous ulcers due to lack of venous return to the heart; this creates a pooling of blood in the lower extremities leading to skin changes. Venous insufficiency results from a failure of or lack of valves in the vein and leads to chronic edema and skin changes that result from hemosiderin deposition. Valves should open and close with each heartbeat, but when they become incompetent and don’t close properly,
- Blood flows backward or in a retrograde fashion, causing pooling in the lower extremity that is affected.
- Hemosiderin develops from red blood cell breakdown in the tissue where blood has leaked from the vascular compartment into the subcutaneous tissue; leaving a brownish stain on the skin when the red blood cells break down and weakens the skin.
- Itching develops and scratching leads to a trauma that initiates breakdown.
- The skin becomes dry and scaly.
- Breakdown may occur as a result of extensive edema, which causes the skin to tear. It may begin with the weeping of the skin due to the stretching but ultimately leads to an ulcer.
- Edema is a result of the accumulation of fluid in the interstitial tissue and leads to changes in skin integrity. This increased interstitial pressure changes how the cells and capillaries function, further delaying the healing process.
- Skin in the lower leg can become fibrotic and is at high risk for injury.
Reduction in these risk factors begins with elevation and compression. When the patient is sitting, teach them to elevate the legs above the level of the hips. If they are lying down, the legs should be above heart level. Leg exercises with flexion and extension of the ankles will help to activate the calf muscle pump and aid in venous return to the heart. Skincare is critical to promote healing venous wounds and to prevent a recurrence. Some patients may need topical steroids for stasis dermatitis. Regular use of moisturizers is important in this patient as well and again should be fragrance-free. In addition to elevation, compression will help to overcome some of the barriers to wound healing when edema is present. Compression should fit firmly with the tightest compression at the ankle.
Immunosuppression
Patients who are immunocompromised may experience delayed wound healing due to the decrease in the inflammatory phase of healing. They are also at risk for the development of chronic wounds as well as wound infection. Patients in this category include any patient on systemic steroid therapy, such as those who have transplants, rheumatoid arthritis, pulmonary disease, or other connective tissue disorders. Steroids can slow the inflammatory phase of wound healing and keep them from progressing through the normal stages of wound healing. Conversely, some topical steroids have been used with some success to treat chronic wounds.
Patients on chemotherapy may experience delayed wound healing through effects on vascular endothelial growth factor. This factor plays a role in angiogenesis in the early stages of wound healing. Unfortunately, this factor is a target for cancer therapy. Chemotherapy is also known to lead to neuropathy which places a patient at higher risk for loss of sensation. Radiation therapy can also produce delayed wound healing, especially when administered in an area of a recent incision or in the skin where an incision may need to be placed. These wounds are more likely to develop complications. Radiation causes ischemic changes in the skin and may lead to ulcers that take a very long time to heal. Patient education for these patients involves making sure they are eating a well-balanced diet to provide proper nutrition and keeping skin moisturized. This may be challenging in the patient undergoing chemotherapy; protein supplements may be needed for nutrition (3).
Obesity
Delayed wound healing in obese individuals is related to many factors. The additional adipose tissue has reduced vascular flow as there are fewer vessels found in subcutaneous tissue. Wound tension is increased. Decreased perfusion to the skin increases the susceptibility to pressure ulcers. Patients may also be less mobile and unable to change position frequently. They are also at higher risk for skin friction when moving. Counseling patients regarding diet and exercise is vital, but patience is of the utmost importance as weight loss is a slow process (3).
Wound Assessment
History and Physical
Wound assessment begins with a complete history and physical exam. What do I need to know about this patient to help me understand why they have a wound and how to treat it? These are the following questions in the assessment process to help you determine a treatment plan.
- When did it start?
- What happened to lead to the wound?
- What is the patient doing currently to treat the wound?
- What has been tried before?
- Is there pain? Is there no pain?
- Is this a wound that went away and came back?
- What healed it last time?
- What other medical conditions or risk factors are present that may impact healing?
- Do they smoke?
- Do they have help to care for themselves?
- Are they ambulatory or need assistive devices?
- Do they work?
- What is their surgical history?
- What diagnostic studies have been performed?
All this information will help in knowing how to proceed and how to educate the patient as the process moves forward (5, 9).
Wound Examination
Look at the wound and determine the condition of the bed, size of the wound, and condition of the skin around it. Is there an infection? For a surgical wound, are the edges together leaking or red? Documentation should include measurements that include length, width, and depth in centimeters—document how the wound is measured. For example, use the head as 12:00 and measure the length in this dimension and the width from 9:00 across to 3:00. Measure in the same plane every time the wound is measured. This is especially critical if you are not the same one seeing the patient at every visit. Depth should include the depth from the surface of the wound to the bottom and any undermining or tunneling found in the wound. Looking at the wound edges and the surrounding skin will help guide the management of the wound itself. Wound edges may have a rolled-up appearance or contain callus. If the documentation system allows, “a picture is worth a thousand words,” (9).
Describing the Wound
This can be challenging unless you know what all the words mean, so let’s break it down to make it easier to understand. These terms will give those who read the documentation a good picture of what is going on with the wound and help guide the choices made for management and wound healing (10).
- Exudate/maceration/purulence – drainage/white areas due to excessive moisture on the skin/thick yellow exudate indicating infection
- Slough – thick yellow tissue that slows wound healing and needs to be removed by debridement
- Necrosis/Eschar – dead tissue over a wound that may hide the true extent of the wound
- Erythema/Induration – redness around the wound/hardened tissue associated with an increase in fibrin and inflammation
- Undermining/tunneling – tissue under the wound edges becomes eroded/channels that extend deep into a wound
- Granulation tissue – new tissue with microscopic blood vessels and connective tissue
- Hypergranulation – excessive granulation tissue formation beyond the edges of a wound
Wound Management
We previously discussed what delays wound healing, so let’s review the mandatory requirements. A wound must have these things to heal:
- Have adequate blood flow.
- Be clear of necrotic tissue and slough.
- Be infection free and be kept moist.
When a wound becomes chronic, wound care changes. Choosing the proper wound dressing aids in the healing process. Dressings are chosen with the following in mind:
- Dead space must be eliminated
- Exudate must be controlled
- Bacterial overgrowth should be minimized
- Proper fluid balance should be maintained
- Protection is provided and bacteria are kept out
- Costs must be contained
- Dressings must be manageable for the patient/caregiver/nurses including reduction of pain and fewer changes (9, 11)
Medical Management
We have already talked about some, but let’s dive in a little deeper to talk about managing a few of those things. Managing infection is key to making sure that healing will continue once a wound has developed. If you could put every wound under a microscope, you would see bacteria in every open wound. They live everywhere and we can’t keep them out of the wound, but remember that every wound is not infected, and antibiotic therapy should be reserved for the wound that is showing other signs of infection. Things that indicate an infected wound include purulent drainage, odor, cellulitis, fever, chills, and difficulty controlling blood sugar. Advanced signs would include hypotension, osteomyelitis, and nausea; treatment of infection may begin empirically. This is using the antibiotic that would most likely cover what is suspected to be in the wound. Ultimately, the antibiotic therapy should be based on culture results so that any unusual bacteria may be detected and treated appropriately. Targeting bacteria with culture results will help to reduce the development of resistant bacteria. Treatment of infection has become much more challenging in recent years due to the development of resistance. It’s critical to use good stewardship with antibiotics to help control resistance (11).
Managing blood sugar will be of utmost importance if the wound patient is a diabetic. Blood sugar that is out of control will hinder wound healing and also predisposes the patient to infection. Remember that challenges with blood sugar control in someone who has been fairly well controlled may be a sign of infection and should be followed up. Encourage patients to check their blood sugar regularly during wound management. This will help them to see what is happening and correct any issues they may be having with wound healing that is related to diabetes. The A1C changes slowly so help them understand that they need to know daily what is going on with their blood sugar to catch any issues early (11).
Self Quiz
Ask yourself...
A patient’s A1C last week was 9, and his diabetic foot ulcer has almost stopped showing any signs of progress. What education does this patient need while trying to get this diabetic foot ulcer healed?
What other steps may be needed to determine why the wound is not healing?
What contributed to the rise in Ms. E’s A1C from 10.7 to 12 over the six-month period of wound care she has been undergoing?
Wound Management (cont.)
Role of Debridement
One of the things that will deter a wound from healing is the presence of devitalized tissue. This is tissue in the wound that builds up on the surface of the wound and is also known as slough. It is made up of fibrin with some dead cells and leukocytes; it can develop into necrotic tissue. This buildup can lead to biofilm and will stop a wound dead in its tracks. That wound needs angiogenesis to get that new tissue to form, and biofilm won’t let this happen. The biofilm is a bacterial overgrowth that forms on the surface of the wound. To keep the surface of the wound fresh and moving forward, serial debridement is needed. Think of this chronic wound as being sluggish because this slough and necrosis make the body lazy in a way, and it thinks, “Wow, I don’t have to work so hard now.” Debridement wakes the wound by telling it there is more work to do, and now it thinks, “Hey, we have an acute wound, let’s get going. We have a new wound to get healed,” (9, 11).
Debridement is usually done with a sharp instrument, but there are enzymatic products that can be used for extensive slough in a patient who may not tolerate the sharp debridement. Sharp debridement removes excess slough, necrotic areas and keeps the edges of the wound fresh, so they continue granulating toward the center to heal a wound. Debridement preps the wound for the dressing and for the use of biologics that may be needed to speed wound healing. Part of debriding the wound includes irrigation to remove loose tissue from the surface, which also helps remove bacteria. This can be done with a syringe and saline or with a pulse lavage device if it is available. Typically, saline is the solution of choice. Some commercial preparations are available in a pump spray bottle as well. For patients that have painful wounds, some clinicians (this author included) will use lidocaine gel or another topical anesthetic in the wound to provide anesthetization of the wound prior to debridement to help the patient tolerate the procedure. For wounds that are insensate, such as diabetic foot wounds, no topical agent is needed (9, 11).
Case Study Update
Ms. E began undergoing serial debridements early in her post-op course. They were done in the office and initially with the aid of topical anesthetic to help with pain control. As the process went forward, she no longer needed an anesthetic. This may happen due to tolerance of the procedure or lack of sensation in the new tissue that is forming. In this case, it was most likely due to beginning the use of the skin substitute, which covered the open nerve endings in the base of the wound. This is seen frequently in the author’s practice when using skin substitutes.
Due to the size of the wound, Kerecis was started to try to decrease the time it would take to heal this very large wound. This skin substitute was applied weekly in the office, and NPWT was placed over the wound. She did not require dressing changes outside the office as the dressing is left in place for the full week between visits. Due to her lack of adherence to the plan of care and continuing to engage in activities that she was counseled not to do, there were significant issues with keeping the dressing in place, further slowing the healing process. When the NPWT was not in place, the wound was exposed to too much moisture from excessive exudate, causing maceration of the lower half of the wound. Fortunately, she ultimately got better at keeping the dressing in place.
Self Quiz
Ask yourself...
What techniques can be used to help patients tolerate wound debridement?
Is there anything that can be done ahead of time to prepare the patient for the procedure?
What other advantages may exist in the patient whose dressing is only changed weekly in the office?
Wound Management (cont.)
Treating Dead Space
In wounds that have cavities known as dead space, it is vital that these areas be filled to absorb any fluid in the wound and provide an environment for ongoing granulation in the dead space. Traditionally, large cavity wounds have been packed with saline moistened gauze to fill areas of undermining or tunneling and then covered with dry gauze. These dressing changes must be frequent to prevent the gauze from completely drying out; this may be as much as three times a day. If it is a painful wound, this can be very traumatic to the patient. Unfortunately, this may also pull out granulation tissue and reinjure the healthy tissue forming in the wound. This technique should be used only for a short time in wounds that have significant slough and necrosis. Once it is removed, the dressing should be changed to another regimen. In cases where the wound is painful and frequent dressings are required, a permeable silicone dressing may be placed in the base of the wound and left in place up to seven days to decrease the gauze dressing’s adherence to healthy tissue. These dressings allow exudate to be absorbed and slough to be removed but protect granulation in the base of the wound (9, 11).
A good option for large wounds with dead space is to use negative pressure wound therapy (NPWT) if it is available. This therapy is especially valuable in very large open wounds that have large amounts of exudate. It has been shown to reduce edema in peri-wound skin as well as stimulate circulation in the wound, helping with angiogenesis which leads to improvement in granulation tissue formation. All that fluid draining from the wound is suctioned into the container which keeps excessive moisture away from the wound. There are different types of foam available for NPWT that allow for packing into smaller tunnels and areas of undermining. For painful wounds, this also reduces the number of times the dressing requires changing as most NPWT treatments involve changes three times weekly. The same silicone barrier that can be used in the gauze dressing can be placed under the foam for NPWT if the wound is extremely painful. When using NPWT for treatment, patients will need to be made aware of the odor that accompanies this treatment when there is a large amount of drainage. Reassure them that this is normal and does not necessarily indicate that there is anything wrong with the wound (9, 11).
Other Medical Treatments
Other things that may be used for wounds include growth factors, iodine-based dressings, silver dressings, and honey. Growth factors may be platelet-derived, epidermal, or granulocyte-macrophage colony-stimulating. Cadoexomer iodine helps to reduce the bacterial load in a wound and provides a moist environment. It is used for short periods of time. Many dressings now can be found with silver which is known to be toxic to bacteria. Study results, however, have not shown this to be superior to standard therapy. It is still used as it may reduce contamination by bacteria on the surface of the wound. Honey is probably the oldest known wound preparation, dating back to ancient times. It carries broad-spectrum antimicrobial properties. This is due to its high osmolarity and because it is concentrated with hydrogen peroxide. It is not used in all wounds, but there are situations where it is very valuable, such as burns or small wounds that need moisture to keep the healing process moving forward. Topical beta-blockers are being studied, but evidence supporting their efficacy is limited (11).
Some wounds may benefit from additional therapies such as hyperbaric oxygen, low-frequency ultrasound, electrical stimulation, electromagnetic therapy, and phototherapy. Not every location may have access to these therapies, but they may prove useful when available in various types of wounds. Treatment of hypergranulation tissue may be needed and is usually done by a wound specialist. This may involve topical steroids or, in some cases, silver nitrate; these treatments are to be used with caution. Applying pressure to a wound may also aid in reducing hypergranulation tissue (11, 12).
Choosing the Right Dressing
There are many types of dressings to choose from when it comes to caring for a wound. And many are specific to each wound type. The first step in considering which dressing is best is to look for moisture control properties. Remember that wound you have seen that was so wet the skin was macerated around the edges? That wound won’t heal because it is way too wet. Or the wound that was so dry that the dressing was stuck to the bottom of it? This wound won’t progress either. Gone are the days when the wound should be “left open to air.” Studies have shown that occluded wounds heal up to 40 percent faster. Theories as to why include leaving the wound in its own fluid which is rich in its own growth factors, and epidermal cells migrate easier. This is truer in the acute wound than in the chronic wound. Occluded wounds may have less significant scarring depending on the size of the wound (11).
So, the first choice is to look for something that will provide moisture balance and keep that excessive drainage away from the wound while maintaining a good level of moisture. Remember, wounds need moisture balance. Most of these dressings allow for daily changes, reducing the time the wound is open and helps with pain control for those very painful wounds. There is no ideal dressing, so looking at what’s available will help to determine what’s best for each type of wound.
Dressing Types (12):
Open: This is the gauze dressing that comes in many forms, from different size pads to different size rolls. They are inexpensive and can be used to pack large wounds but require frequent changes.
Semi-open: This category includes impregnated mesh gauze such as Vaseline gauze and Xeroform. They are inexpensive and easy to use. They do not, however, control exudate, nor do they maintain moisture in the wound. They also require frequent changes.
Semi-occlusive: This category includes foams, films, alginates, hydrogels, and hydrocolloids.
Films will allow oxygen in but will keep bacteria out and include products such as Tegaderm, Opsite, and Bioclusive products. These are great for IV sites and donor sites for skin grafts. They maintain moisture and are transparent and self-adhesive. They do not absorb drainage and can lead to maceration if there is too much drainage in a wound. They should not be left in place as a wound becomes drier as they may cause damage upon removal.
Foams are two-layer products with a foam layer that lays against the wound and backing to prevent drainage from leaking out and bacteria from entering the wound. These include Allevyn, Mepilex, Lyofoam, and Spyrosorb. They can absorb fluid and conform easily to wounds so they can be used as filler for dead space. They are opaque and may need to be changed more frequently in heavily exudating wounds. They should not be used on wounds with little moisture as they can further dry out a wound; additionally, they can be used on skin tears as well.
Alginates are made from various forms of algae. In the presence of wound fluids, they form a gel that helps to cover and even pack a wound. There are many forms of alginates to help customize the dressing, such as pads, ropes, and beads. They are great for moderate to heavy wound drainage and can remain in place for several days. They require a secondary dressing over them and can dry out a wound that does not have enough moisture. Unfortunately, they also have an unpleasant odor when changing the bandage.
Hydrocolloids consist of a gel or a foam with a self-adhesive film creating a moist environment. They provide a gentle debridement when removed from the wound and can be used for packing wounds in some instances. They, unfortunately, can create an odor and may need daily changes. They include products such as Duoderm, Tegasorb, J and J Ulcer dressing, and Comfeel. Cadoexemer iodine falls in this category of wound dressing as well. This form of iodine disperses slowly so as not to cause tissue damage. It comes in a paste or a sheet form that can be cut to fit a wound.
Hydrogels are made of synthetic polymers that are mostly water and come in sheets, gels, or foams. They can absorb or donate water to the wound and include Intrasite Gel, Carrington Gel, and Elastogel. They are most often used for dry wounds and can be cooling to the wound, reducing pain. There are no significant disadvantages but have been shown to allow gram-negative bacteria to grow (11).
Ongoing Trauma
During the healing process, wounds are very susceptible to trauma as the fragile tissue is working to epithelialize and granulate. Protecting wounds from trauma is critical. Venous wounds may itch and the patient will want to scratch the wound and the peri-wound skin. Prevention of scratching will help reduce bacteria on the skin as well as reduce the chance of new ulcer formation in the skin that is very susceptible to injury. Diabetic ulcers are most commonly on the bottom of the foot, and if they are not offloaded, they will have little chance of healing. Patients may need offloading shoes or other means of stopping the friction that walking creates on the bottom of the foot. Other options include Cam walkers, total contact casts, knee scooters, crutches, wheelchairs, and bed rest. Patients must understand that even a few steps can undo what the body has worked days or weeks to rebuild. Once the wound is healed, diabetic patients will need long-term use of proper footwear to prevent a recurrence (8, 13).
Managing Other Issues (14)
Odor: Managing odor can be accomplished through regular debridement to reduce the bacterial burden in the wound as well as using charcoal dressings and soaks such as acetic acid or Dakin’s.
Bleeding: Bleeding may occur in malignant wounds, after debridement, or in patients on chronic anticoagulation therapy. Pressure to the wound is usually enough to stop oozing. Agents can be applied to the wound that provides hemostasis, or it may be done with silver nitrate, cautery, or infiltration with epinephrine if more significant.
Itching: This is usually more common in skin that is dry or if dermatitis is present. Moisturizers and skin protection is key. In some instances, a topical steroid cream may be needed. Help patients understand that dry skin is not healthy and can break down, leading to the entry of bacteria, resulting in cellulitis.
Pain: Pain control is critical to helping a patient follow the medical regimen and being able to tolerate dressing changes. Teach patients to take pain medications prior to dressing changes. The use of topical anesthetics may also be of help during debridement.
Edema: If edema is not controlled, the wound will have difficulty healing. With a wound present, other options besides compression stockings will need to be selected. Among these are Tubi-grip, Circaid wraps, Unna boots, and 2-layer compression wraps. Any of these can be used over the bandage for most patients. Elevation must also be used in conjunction with compression to gain the full benefit of medical management. A good rule to remember is “toes above the nose” (author quote) to get the maximum benefit from elevation. This is sometimes a challenge for the patient with COPD, CHF, obesity, or any condition that prohibits them from reclining far enough to get the legs high enough to decrease edema (13).
Self Quiz
Ask yourself...
What methods of elevation may be used for the patient with medical conditions that hinder them from lying flat?
What wounds tend to be the most painful?
What can be happening in a wound that develops an odor that was not present at the last assessment?
Surgical Management
Some wounds will require surgical management to get them back on track. Extensive debridement may be necessary to remove deep infection, gangrenous areas, devitalized or infected bone, or foreign bodies. Patients that cannot tolerate sufficient outpatient debridement or require bone biopsy may also need operative debridement. If blood flow is an issue, revascularization will be needed. For diabetic foot wounds, surgery may be needed to correct bony abnormalities. Venous ulcers may need surgical ablation to reduce pressure related to venous insufficiency for the ulcer to heal. Some wounds, such as pressure ulcers, may be large enough to require skin or muscle flaps to close. If pressure ulcers are being exposed to fecal material, a diverting colostomy may be necessary (11, 16).
Summary
Wound care is a challenging process, and nurses must consider many factors to promote healing in an optimal time. I hope you have learned at least one thing that you did not know about wound care, and the next complex issue you have with your wound care patients will be made easier by what you have learned.
References + Disclaimer
- Armstrong, D. (2020, July 20). Basic principles of wound healing [Review of Basic principles of wound healing]. Www.uptodate.com; Wolters Kluwer. Accessed 3/14/2021.
- Nettina, S. M. (2019). Lippincott manual of nursing practice. Wolters Kluwer.
- Armstrong, D. (2020, February 12). Risk factors for impaired wound healing and wound complications [Review of Risk factors for impaired wound healing and wound complications]. Www.uptodate.com; Wolters Kluwer. Accessed 3/14/2021.
- Anderson, D. (2019, December 18). Antimicrobial prophylaxis for prevention of surgical site infection in adults [Review of Antimicrobial prophylaxis for prevention of surgical site infection in adults]. Www.uptodate.com; Wolters Kluwer. Accessed 3/19/2021.
- Armstrong, D. (2021, February 22). Clinical assessment of chronic wounds [Review of Clinical assessment of chronic wounds]. Www.uptodate.com; Wolters Kluwer. Accessed 3/24/2021.
- (n.d.). Know the real cost of cigarettes [Review of Know the real cost of cigarettes]. Retrieved March 21, 2021, from https://therealcost.betobaccofree.hhs.gov
- (n.d.). Therapeutic shoes and inserts [Review of Therapeutic shoes and inserts]. Retrieved March 21, 2021, from https://www.medicare.gov/coverage/therapeutic-shoes-inserts
- Cynthia Rebik Christensen, Lewis, P. A., & Society For Vascular Nursing. (2014). Core curriculum for vascular nursing. Wolters Kluwer Health ; Philadelphia, Pa.
- Bishop, A. (2021). Wound assessment and dressing selection: an overview. British Journal of Nursing, 30(5), S12–S20. https://doi.org/10.12968/bjon.2021.30.5.s12
- Mahoney, K. (2020). Part 1: wound assessment [Review of Part 1: wound assessment]. JCN, 34(2), 28–35.
- Armstrong, D. (2021, January 12). Basic principles of wound management [Review of Basic principles of wound management]. Www.uptodate.com; Wolters Kluwer. Accessed 3/14/2021.
- Mitchell, A., & Llumigusin, D. (2021). The assessment and management of hypergranulation. British Journal of Nursing, 30(5), S6–S10. https://doi.org/10.12968/bjon.2021.30.5.s6
- Evans, K., & Kim, P. (2020, September 1). Overview of treatment of chronic wounds [Review of Overview of treatment of chronic wounds]. Www.uptodate.com; Wolters Kluwer. Accessed 3/29/2021.
- Shahrokhi, S. (2021, February 22). Skin substitutes [Review of Skin substitutes]. Www.uptodate.com; Wolters Kluwer. Accessed 4/7/2021.
- Winters, C. (2018). Fish skin to heal wounds [Review of Fish skin to heal wounds]. Podiatry Management, 37(9), 119–123.
- Berlowitz, D. (2020, May 12). Clinical staging and management of pressure-induced skin and soft tissue injury [Review of Clinical staging and management of pressure-induced skin and soft tissue injury]. Www.uptodate.com; Wolters Kluwer. Accessed 4/7/2021.
Disclaimer:
Use of Course Content. The courses provided by NCC are based on industry knowledge and input from professional nurses, experts, practitioners, and other individuals and institutions. The information presented in this course is intended solely for the use of healthcare professionals taking this course, for credit, from NCC. The information is designed to assist healthcare professionals, including nurses, in addressing issues associated with healthcare. The information provided in this course is general in nature and is not designed to address any specific situation. This publication in no way absolves facilities of their responsibility for the appropriate orientation of healthcare professionals. Hospitals or other organizations using this publication as a part of their own orientation processes should review the contents of this publication to ensure accuracy and compliance before using this publication. Knowledge, procedures or insight gained from the Student in the course of taking classes provided by NCC may be used at the Student’s discretion during their course of work or otherwise in a professional capacity. The Student understands and agrees that NCC shall not be held liable for any acts, errors, advice or omissions provided by the Student based on knowledge or advice acquired by NCC. The Student is solely responsible for his/her own actions, even if information and/or education was acquired from a NCC course pertaining to that action or actions. By clicking “complete” you are agreeing to these terms of use.
➁ Complete Survey
Give us your thoughts and feedback
➂ Click Complete
To receive your certificate