Course
Triage Nurse: Tips on Pediatric Patients
Course Highlights
- In this course we will learn about assessment guidelines and tools commonly utilized by triage nurses.
- You’ll also learn the basics of age-specific developmental milestones and what signs to look for in pediatric patients presenting to the emergency department.
- You’ll leave this course with a broader understanding of how to care for special pediatric populations as a triage nurse.
About
Contact Hours Awarded: 1.5
Course By:
Katie Maloney
MPH, BSN, RN, CPEN
Begin Now
Read Course | Complete Survey | Claim Credit
➀ Read and Learn
The following course content
Introduction
The word “triage” is derived from the French verb “to sort,” and that is exactly how it is interpreted in medicine today. When looking at the emergency department (ED), the goal of triaging is to identify resources that do the most good for the largest number of ill and injured patients. As EDs have become busier over time, this skill has become a critical piece of providing the highest and most efficient level of care possible; especially with pediatric populations who are not as readily able to voice their symptoms. Learning the cues of specific illnesses, understanding age-specific considerations, and implementing pediatric-specific tools are essential in accurately determining the required level of care and interventions needed in an expeditious manner.
This course will cover evidence-based practices and specific skills that will help triage nurses assess and determine a child’s acuity accurately.

Self Quiz
Ask yourself...
What is your comfort level with pediatric patient populations?
What is your comfort level with emergency room triage?
What is your comfort level with triaging pediatric patients?
What is one thing you hope to learn about the care of pediatric patients in triage in this course?
What are your thoughts on pediatric specific protocols for triage?
Assessment Guidelines for Triage Nurses
Accurate pediatric triage requires a working knowledge of normal vital signs so that aberrancies are easily noted. Additionally, triage nurses should understand the importance of weight in kilograms, as most pediatric medications are weight-based. Embracing these concepts and incorporating them into the triage of each patient will help to deliver excellent care for children and their families.
Assessment details that may alter a child’s vital signs but not necessarily indicate a higher acuity include:
- elevated heart rate while crying and/or febrile
- elevated respiratory rate while febrile, without increased work of breathing
- high blood pressures if moving or agitated (pro-tip: manual BPs are gentler and less anxiety producing for your pediatric buddies and the parent attempting to hold them still and answer your questions)
It is extremely important to recognize the difference in vitals for each age range and how significantly they differ. Take temperature as an example:
- For an infant less than 28 days of life, a worrisome core temperature is greater than 100.4.
- For children three months and over, temperatures above 101 are indicative of the need for evaluation.
- In the neonatal period, a low core temperature, hypothermia can be a symptom of sepsis in this population and warrants further evaluation.
| Age | Heart Rate | Respiratory Rate | Systolic BP | Diastolic BP |
| Neonate (<28 days) | 100-165 bpm | 30-55 | 65-85 | 35-55 |
| Infant (1 month to 1 year) | 100-150 | 30-55 | 80-100 | 55-65 |
| Toddler (1-2 years) | 70-110 | 20-30 | 90-105 | 55-70 |
| Preschool (3-5 years) | 65-110 | 20-25 | 95-107 | 60-71 |
| School Age (6-11 years) | 60-95 | 14-22 | 95-110 | 60-76 |
| Adolescent (12-15 years) | 55-85 | 12-18 | 110-124 | 69-80 |
Self Quiz
Ask yourself...
Consider patients you have seen in your practice: how often has a parent rushed their child to the ED for a fever after only a short period of time and the child is, otherwise, asymptomatic at the time?
After the above reminder, how might you counsel the family regarding fevers in the pediatric population?
PAT Tool
Honing your ability to rapidly identify “sick versus not sick” is critical to becoming an efficient and reliable triage nurse, especially in pediatric populations. A particularly helpful tool for this is the Pediatric Assessment Triangle (PAT) which allows the triage nurse an objective means of determining “sick, sicker, sickest” based upon an initial, across the room assessment of a child. There are three major components involved in this tool:
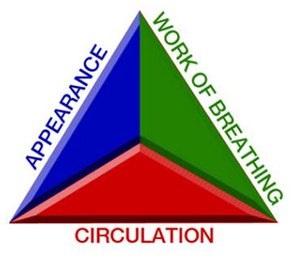
- General appearance.
- Work of breathing
- Circulation to skin (1).
Additionally, the PAT can be employed as a means of reassessment after interventions, as well as ongoing observation of patients while in the waiting room.
Appearance
This PAT component is where the triage nurse considers the overall first impression of the child. This is significant as it offers insight into the adequacy of ventilation, oxygenation, brain perfusion, and cues health care providers toward any dysfunction of the central nervous system (1). This component of the triangle requires the observer to classify the following as appropriateness of the child’s tone:
Assessment of Tone
A child’s tone can vary depending upon their age and baseline stage of development. Knowledge of some innate reflexes in infancy assists the triage nurse in determining an ill or injured infant versus a healthy infant. The Moro, or startle reflex, is an excellent and simple test to perform and can be elicited by placing them on a cold surface from their caregiver’s arms; a scale is a great option for this test as it allows the provider to gain necessary vitals as well as assess tone.
Assess the infant for extension and stretching of extremities outward from the core. This is usually accompanied by a cry which will assist with strength and pitch of cry, which is another aspect within the Appearance section of the PAT.
Can they sit upright unsupported? If not, is this their baseline or a deviation from such? Are they moving all four extremities with adequate strength and coordination? Do they have any unilateral or bilateral stiffening or flaccidity that is not their baseline?
Assessment of Activity Level
This assessment can be relatively simple with toddlers and older children.
Are they playful and interactive with caregivers? Are they ambulatory on their own?
Understanding a few key motor milestones for infants will aid in the determination of appropriateness for age: infants without motor deficits should roll over and sit up at three–to–five months of age, crawl at or around six–to–nine months, and walk or cruise around furniture at about one year (3).
Assessment of Gaze
This form of assessment is easy for triage nurses and can be done from across a room if needed. If a child is not spontaneously opening their eyes in triage, this should indicate some need for immediate intervention. The underlying pathology might not be immediately clear, but the experienced triage nurse recognizes that this could be an indication of serious illness that warrants further evaluation.
Infants may require stimuli, either verbal or tactile, to allow for spontaneous eye-opening but once stimulated, they should readily open their eyes. For a general point of reference: a healthy, developmentally appropriate infant should track and follow with their gaze by the age of three months.
Does the child have any dysconjugate gaze or abnormal eye movements? If age-appropriate, are they tracking their caregiver’s face? Do they make eye contact with their caregiver? Any abnormality of eye movement should raise concern for the knowledgeable triage nurse, as should any unwillingness to make or maintain eye contact in the older child.
Consolability
Consolability is a significant indicator of wellness and central nervous system functioning, especially in the non-verbal infant or child. If an infant is anxious, irritable, and crying with the nurse’s triage interventions but immediately consoles when placed in a caregivers’ arms, this demonstrates appropriate neurological regulation. In contrast, a critically ill or injured child will have little or no response to attempts at consoling and soothing measures, and this may indicate a need to intervene and either relieve a pain source or assess for some underlying process.
Work of Breathing
The second component of the PAT that triage nurses should utilize is “Work of Breathing.“ The best means of assessing a pediatric patient’s work of breathing is to ensure they are in the position of greatest comfort. It is often the easiest means to gather medical history from caregivers while simultaneously observing the rate, depth, and quality of respirations in the child. Looking and listening from across the room offers the greatest level of insight for the triage nurse into the adequacy of oxygenation and ventilation: abnormal airway noises, abnormal positioning (i.e., tripoding), retractions, and/or nasal flaring are all red flags of significant distress (1).
Circulation
The third and final component of the PAT is “Circulation to Skin.” A child’s central color as well as color of lips and mucous membranes are important indicators of adequate cardiac output, as well as perfusion of central and end organs (1). Significant indicators of poor perfusion include pallor, cyanosis, mottling- with central mottling being a grave prognostic indicator.
Infants will often have peripheral mottling in response to cold exposure, so ensuring that it resolves with warming measures (requesting caregiver swaddle child) is an important visual indicator of adequate perfusion. In addition, the febrile child may have peripheral mottling related to tachycardia and shunting blood to vital organs.
This finding should indicate the need for further evaluation; however, in this circumstance, does not necessarily indicate a functional pump problem.
Application of the PAT for Triage Nurses
The process of triage nurses utilizing the PAT serves as the cornerstone to rapid identification of the sicker and sickest pediatric patients that may require immediate interventions. This determination can lead to the prevention of poor outcomes. If done correctly, it should take no more than 30 seconds to accurately identify the child in greatest need of care.
Generally, an abnormality within the assessment of any one component of the PAT indicates that the child requires initiation of a focused assessment immediately. An abnormality of two or more components, indicates that the patient requires rapid resuscitation and should be moved to an area that allows for such (1).
There are several other “pediatric red flags” that the prudent triage nurse should commit to memory. Breaking these down into the ABCs of the emergency nursing pediatric process, they include (1):
- Airway: apnea, choking, drooling, or any audible adventitious airway noise
- Breathing: grunting, retractions noted to sternal muscles indicating increased work of breathing, irregular breathing patterns, a respiratory rate of >60 or <20 in children less than six years old, any focal absence of breath sounds, and cyanosis, nasal flaring, or grunting
- Circulatory: cool or clammy skin, bradycardia (heart rate <60 beats per minute), tachycardia (heart rate >200 beats per minute), diminished or absent peripheral pulses, decreased tearing
- Disability: altered level of consciousness based on age, inconsolability, and sunken or bulging fontanel in infants
- Exposure: petechia, purpura, and any abnormal bruising patterns- especially on unanticipated areas such as trunk, torso, backs of ears, backs of legs, and with suspicious patterning
- Vital Signs: Hypothermia in any age, fever in infant less than 3 months (>100.4 F) and temperature greater than 104-105 F in any age
- History: history of chronic illness or family crisis, or any return to the emergency department within 24 hours
Acknowledging the above pediatric red flags and utilizing the PAT as a guide, how would you categorize the three different children in the triage scenarios below?
Scenarios for Knowledge Integration
Scenario 1:
A three-year-old with a history of reactive airway disease presents to triage with complaints of coughing for two days. She is awake, alert, and smiling at her mother. She has mild tracheal tugging, no audible adventitious airway noises, and a respiratory rate of twenty-four. Her lips are pink, as are her fingertips, and her mucous membranes are also pink and moist.
Scenario 2:
A second child is a 10-month-old without known past medical history. The child had a fall from standing, struck his head on the edge of a coffee table, sustained a 1cm vertical laceration to the mid-forehead 1–hour prior to arrival, and had no loss of consciousness; He is awake and alert with coordinated movements of extremities, no dysconjugate gaze, crying in triage, but consolable with mother. He is breathing at a normal rate and depth when calm, with no outward signs of bleeding, and has pink and warm skin.
Scenario 3:
The final child is a 3-month-old with a history of term–birth which is still in his car seat. The mother reports he has had difficulty feeding for over a month now, including irritability, sweating, and increased work of breathing. In the last 48 hours, she has noticed that he is more fussy than usual and will not take a bottle; also, she has noticed noisy breathing at rest and some swelling to his hands and feet. As the triage nurse, during your across–the–room assessment, you notice that the infant is awake, occasionally crying, but it sounds weak. You note grunting noises with respirations and a respiratory rate of 70. It is noted as is circumoral and periorbital pallor that turns dusky with crying.
Which child is sick, sicker, and sickest?
Recalling that the child without significant alteration in any one category of the PAT can have their focused assessment deferred (sick), an alteration in one category indicates a need for emergent focused assessment (sicker), and an alteration in two or more of the three categories indicates the need for resuscitation (sickest).
Rationale
The child from scenario 1 has a normal general appearance, a normal rate of respirations for age but tracheal tugging (an indication of increased work of breathing) and normal circulation to their skin.
The second child has a normal general appearance, normal work of breathing, and normal circulation to his skin with bleeding controlled from the head injury.
The final child has an alteration in his general appearance: weak cry, alteration in his work of breathing: grunting respirations, rapid respiratory rate, and alteration in circulation to his skin: circumoral and periorbital duskiness when agitated and pallor at rest.
Based on these findings, the second child is sick, the first is sicker, and the third is the sickest.
Self Quiz
Ask yourself...
- Was there any variation in your categorization of the patients?
- Could the PAT be applied to the adult population as well?
Age-Specific Developmental Milestones
Consideration of age-specific developmental milestones for pediatric patients is another important skill for a triage nurse, as it assists with optimizing the physical assessment.
In the young infant, ensuring their comfort, and using minimal stimulation allows for auscultation of accurate heart tones and breath sounds. This may require allowing the child to remain in the car seat and quietly and gently altering clothing to allow for visualization of the chest wall. Engaging caregiver’s assistance is also advantageous as it offers some element of control for the concerned caregiver while allowing for the best possible exam. You may find that allowing the infant to feed- if medically advisable- will also offer comfort for both caregiver and infant.
In an older infant who can sit unsupported, you can have them sit on the exam table or stretcher; however, you may find increased cooperation if they are left in their caregiver’s arms. Limitation of invasive pieces of the exam should be left until the end to avoid agitation; most older infants find items such as pulse oximetry monitoring devices and blood pressure cuffs to be upsetting, so offering distractions with age-appropriate toys can be helpful.
Toddlers and preschool-aged children learn through play and by doing. Therefore, it is ideal to approach them with an inquisitive and playful perspective if the condition allows (1). They should be allowed choices in positioning for the exam as well as other limited options, but they must allow the patient to feel some sort of control over the situation; engaging the caregiver to participate is also beneficial.
For school-age and adolescent children, their participation will depend largely on the circumstances preceding their presentation to the ED. Independence and privacy are of large importance to both groups and should be considered by the triage nurse whenever possible. To build trust with the pediatric patient it is important to allow them to sit or stand in the position of comfort, undress in privacy, and ensure the most palatable level of caregiver involvement.
Self Quiz
Ask yourself...
Considering the milestones reviewed above, moving forward, how might you alter your practice of triaging specific age groups?
Toddlers can be especially challenging; do you have distraction techniques that you‘ve utilized that have been successful?
If not, is there a way to institute a distraction box for these patients in your facility?
Care of Special Pediatric Populations
The final area we will cover in this course for triage nurses is special pediatric patient populations. Whether you are part of a large, university-associated hospital with a multitude of pediatric resources or a small community-based ED with limited pediatric subspecialists, knowledge of practices specific to special populations will improve the quality of care delivered and improve the experience for the child and their family.
As medicine and technology continues to advance, children with more severe and complex conditions are beginning to live longer; however, the need for greater medical and technological intervention continues to grow. As a triage nurse, it is imperative to acknowledging this need and to be aware of a few key points when these special pediatric populations present to the ED.
First, and foremost, the caregivers for these children are the experts on their condition and the care they require. For this reason, if the acuity of the presenting problem allows, obtaining a thorough medical history as it pertains to the history of present illness is critical to determining the correct interventions. Many families are now seeking medical care with a prepared illness plan from their treatment team. For example, children with alteration in metabolic functioning will often present with a “recipe” of sorts that will identify the intravenous solutions to replete their deficiencies. Ensuring this information accompanies the child back for treatment is essential to optimizing the child’s care plan.
DM Type I with DKA
A common ED visit reason in pediatrics is new-onset Type I Diabetes, often presenting with diabetic ketoacidosis (DKA). Recognition of this in triage can expedite and streamline the care a child will receive.
Presenting symptoms often include:
- Polydipsia
- Polyuria
- Weight loss
- Vomiting
- Fast breathing with Kussmaul Respirations
- Fruity odor in breath
The triage nurse should identify the child who presents with these symptoms as serious, requiring expedited care.
Evaluation of the child’s neurologic state of functioning and obtaining blood glucose as soon as possible should be a critical first step in treating these patients. These symptoms are the human body’s attempt to regulate the hyperglycemia and ketosis occurring as the body breaks down fat. DKA is a medical emergency and requires accurate recognition and quick actions on the part of the first-line care provider- and in this case, usually the triage nurse.
The Septic Neonate
The septic neonate is another pediatric population that requires immediate identification and rapid treatment. For this reason, the triage nurse should be able to identify a neonate at risk for and presenting with the hallmark symptoms of sepsis.
Presenting symptoms often include:
- Feeding difficulties
- Increased sleepiness
- Fever (occasionally)
In other cases, the infant may be hypothermic, which should cause the triage nurse to be suspicious of sepsis and initiate your facility’s pediatric sepsis pathway. The time window for administering antibiotics can have grave consequences for the septic neonate, so triage is a critical piece of expediting care.
Fever and Neutropenia
Fever and neutropenia in the pediatric patient are common presenting problems that require expedited care. As more children are able receive their hematological and oncological treatments as outpatients, the number who require ED visits for treatment-induced neutropenia that develop fevers have increased.
Most caregivers will know to mention their child’s underlying diagnosis, but important pieces for the triage nurse to gather include:
- Time of fever onset
- Last treatment date
- CBC results if known.
Like the septic neonate, the time window for administering antibiotics is critical and should be recognized and coordinated at the point of triage.
Ingestions
Accidental or intentional ingestions are another frequent chief complaint for the pediatric patient population in the ED. Key details to assist with determining the need for immediate interventions include:
- the time of ingestion
- any contact with the poison control center and their recommendations,
- any attempted treatments prior to arrival (especially if vomiting was induced as this could indicate concern for aspiration, retraumatization to esophagus and airway if substance is caustic)
- ingredients of the product or the number of the medication in a bottle prior to ingestion and the dosage of the contents
Your facility providing a reference list of the most dangerous substances as well as allowing access to your designated poison control center are essential resources for a triage nurse. This is important to mention as the recommendations are constantly changing. For example, household bleach is rarely toxic as the FDA has regulated its alkalinity; however, industrial bleach has higher concentrations, and thus, remains very caustic. Distinguishing the details of the ingestant is imperative to accurate care.
Hydrocarbons are another dangerous household products. These are products such as liquid lamp oil, furniture polishes, lighter fluid, and aerosol propellants (1). Unfortunately, these products are usually marketed in enticing colors and often catch the eye of children. The unintentional ingestion of a hydrocarbon causes gastrointestinal distress and severe respiratory impairment if aspirated. Following, if untreated, it can often lead to chemical pneumonitis and the viscosity of the liquid leads to significant lung injury. The biggest risk is that if the child coughs or vomits during or following ingestion, this can lead to a critical illness. If a child is suspected of having ingested a hydrocarbon and continues to have a cough or throat clearing, they require immediate care, including a chest radiograph.
Autism Spectrum Disorder (ASD)
As triage nurses, our focus must be to perform accurate and rapid assessments as well as proper categorization of illness acuity.
When it comes to the care of the pediatric patient with ASD, understanding the stimuli that are most noxious, attempting to alleviate fears, and remaining calm and comforting must be first line treatment. The caregivers of the child and will be your guide to the history of the patient, and potentially, your interpreter depending on the capabilities of the child. Requesting the caregiver’s advice on the best means of performing assessments and how to achieve the child‘s cooperation will lead to a better experience. It may also be useful to assemble a “sensory box“ filled with items such as weighted blankets, light spinners, vibrating rings and other items that can be found through online resources.
Self Quiz
Ask yourself...
Consider the highest acuity pediatric populations you have seen in your practice. Incorporating the above teaching points, is there anything you might alter in your care after this review?
Are there protocols in place to expedite the care of fragile pediatric patient populations?
Conclusion
Triage nurses are the gatekeepers and resource allocators of the ED, so it is of the utmost importance that they are well-informed of the various aspects of assessment tools, care plans for special pediatric populations, and much more; it will ensure the highest possible level of care to the greatest number of patients. Pediatric patients and their families deserve a healthcare provider who is well versed, comfortable with, and confident in their abilities to adequately recognize and appropriately categorize a wide variety of pediatric ill and injured patients.
References + Disclaimer
- Hohenhaus, MA, RN, CEN, FAEN, S. M. (2012). Prioritization: Focused Assessment, Triage, and Decision Making. In Emergency Nursing Pediatric Course, Provider Manual, Fourth Edition (pp. 54-61). Emergency Nurses Association.
- Mersch, MD, FAAP, J. (2020, 11 5). Pediatric Vital Signs Ranges and Charts. EMedicine Health. Retrieved April 5, 2021, from https://www.emedicinehealth.com/pediatric_vital_signs/article_em.htm.
- Patrick, MD, FAEMS, C. (2020, October 27). The Pediatric General Assessment Triangle. EMS Neonatal Pediatrics. Retrieved April 1, 2021, from https://www.ems1.com/ems-products/neonatal-pediatric/articles/the-pediatric-general-assessment-triangle-KE8VtMVnpbpRIJgh/
Disclaimer:
Use of Course Content. The courses provided by NCC are based on industry knowledge and input from professional nurses, experts, practitioners, and other individuals and institutions. The information presented in this course is intended solely for the use of healthcare professionals taking this course, for credit, from NCC. The information is designed to assist healthcare professionals, including nurses, in addressing issues associated with healthcare. The information provided in this course is general in nature and is not designed to address any specific situation. This publication in no way absolves facilities of their responsibility for the appropriate orientation of healthcare professionals. Hospitals or other organizations using this publication as a part of their own orientation processes should review the contents of this publication to ensure accuracy and compliance before using this publication. Knowledge, procedures or insight gained from the Student in the course of taking classes provided by NCC may be used at the Student’s discretion during their course of work or otherwise in a professional capacity. The Student understands and agrees that NCC shall not be held liable for any acts, errors, advice or omissions provided by the Student based on knowledge or advice acquired by NCC. The Student is solely responsible for his/her own actions, even if information and/or education was acquired from a NCC course pertaining to that action or actions. By clicking “complete” you are agreeing to these terms of use.
➁ Complete Survey
Give us your thoughts and feedback
➂ Click Complete
To receive your certificate